ARTICLE
Vol. 134 No. 1535 |
Te Tiriti o Waitangi compliance in regulated health practitioner competency documents in Aotearoa
The health of Māori is a taonga (something treasured and valuable).
Full article available to subscribers
The health of Māori is a taonga (something treasured and valuable).1 As with other Indigenous peoples, Māori experience a disproportionate burden of disease.2 These inequities are fuelled by the intergenerational legacies of colonisation and historical and contemporary manifestations of institutional racism.3 Alongside the Declaration on the Rights of Indigenous Peoples,4 which reaffirms the rights of Indigenous peoples to health, in Aotearoa there is also te Tiriti o Waitangi (te Tiriti), which was in part negotiated to protect Māori health.1
Te Tiriti o Waitangi (Māori text), which was negotiated between the British Crown and hapū (Māori sub-tribes), is the founding document of the colonial state of New Zealand. This unique treaty granted the British the right to govern their people in Aotearoa, reaffirmed Māori tino rangatiratanga (absolute sovereignty), gave Māori equal citizenship rights and guaranteed religious freedom.5 This meant the protection of Māori domain over land, resources and aspirations. Te Tiriti was signed by William Hobson (the Queen’s representative) and more than 500 rangatira (chiefs), and it is recognised under the legal doctrine of contra proferentem as the authoritative text.6
The existence of the Treaty of Waitangi (the Treaty (English version)) has historically created confusion due to the widely held interpretation that Māori ceded sovereignty, despite the Māori version clearly reaffirming Māori tino rangatiratanga. The authors maintain that repeated references by the Crown (the Government) to the English version and the unilateral development of ‘Treaty principles’7 has created a systematic process of disinformation that serves to protect the status quo and the Crown’s assumption of unitary parliamentary sovereignty. This confusion was institutionalised in the Treaty of Waitangi Act 1975, which enables investigation of breaches of both te Tiriti and the Treaty, undermining the definitive position of the Māori text.
Within the health sector, the New Zealand Public Health and Disability Act 2000 refers to the Treaty and, more specifically, to the Treaty principles of partnership, protection and participation.8 Most health policy refers to the Treaty and/or Treaty principles rather than te Tiriti.9 The disinformation continues with the recent Cabinet Office10 circular that affirmed the central place of the Treaty rather than te Tiriti in contemporary public policy.
In clear deference to the Māori text, the Waitangi Tribunal in 2014 (WAI 1040)11 ruled that, by signing te Tiriti, Ngāpuhi (a major northern tribal confederation) did not cede sovereignty. More recently the Waitangi Tribunal ruled (WAI 2575) that key health legislation and policy were not Treaty and/or te Tiriti compliant.12 With a major review of the health sector underway,13 it is timely to re-examine regulated health professionals’ competency documents in relation to their compliance with te Tiriti.
Methods
Regulated health professionals are identified within the Health Practitioners Competence Assurance Act 2003, the Medical Practitioners Act 2007 and the Social Workers Registration Legislation Act 2019. Under this legislation, practitioners are expected to be accountable to their professional authorities and be competent to practice. Annual practising certificates are issued to ensure practitioners work within their professional scope of practice. The 18 professional groups covered by these Acts are chiropractors, dental practitioners, dietitians, medical practitioners, medical radiation technologists, medical technicians, midwives, nurses, occupational therapists, optometrists and dispensing opticians, osteopaths, physiotherapists, pharmacists, podiatrists, psychologists, social workers and psychotherapists.
Following up on Heke, Wilson and Came’s14 examination of regulated health practitioners’ cultural competencies, this paper examined more deeply their engagement specifically with te Tiriti. Core competency documents for the database were collected from the websites of regulated health professional bodies in November–December 2019.
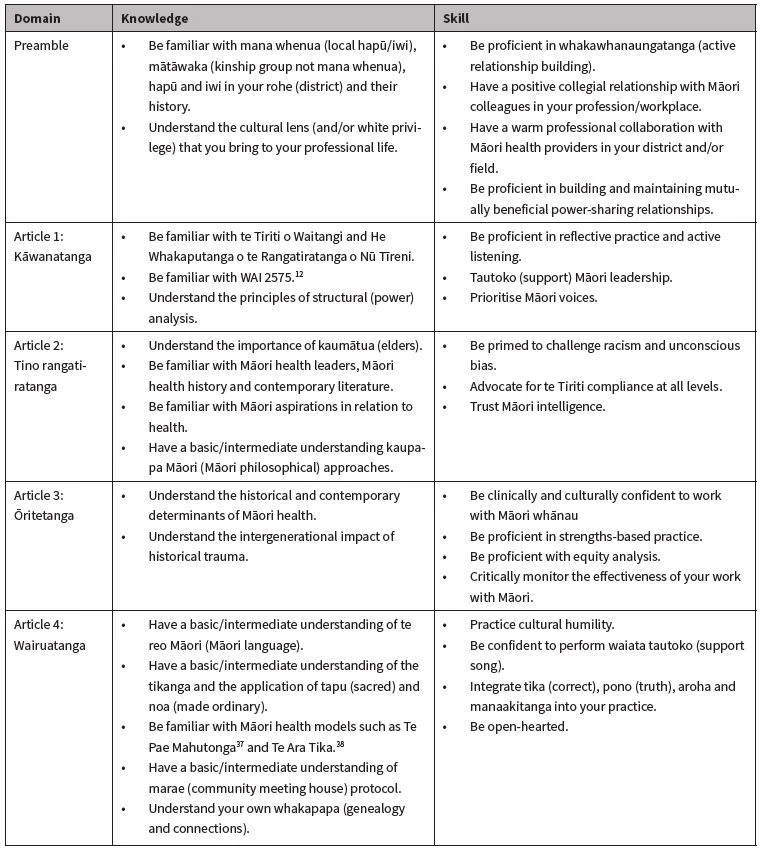
We adopted a five-phase Critical te Tiriti Analysis (CTA)15 to assess te Tiriti compliance of the regulated competency documents. The first phase involved orientating how the competencies address Māori health with reference to priorities, language and epistemologies and how they reflect tino rangatiratanga, Māori citizenship and ōritetanga (equity). The second phase was a close examination on engagement with the five domains (preamble and four articles) of te Tiriti (Table 1).
Table 1: Critical te Tiriti Analysis indicators.15

Phase three involved a determination of competency development, performance and evaluation on a Likert-type five-point rating scale (poor, uncertain, fair, good, excellent) across each of the five domains. Phase four involved identifying how the competencies could be strengthened. Phase five involved a final Māori critique.
In terms of competency documents, we prioritised using core competency documents rather than any peripherally positioned cultural competency/safety or Māori health documents.
Results
Phase one: competency orientation
The collection of competencies we reviewed were published between 2003 and 2019. There was diverse usage of the terms ‘the Treaty’, ‘te Tiriti’ and/or ‘the Treaty principles’. The core competency documents of optometrists/opticians and dentistry make no mention of te Tiriti, the Treaty or Treaty principles. Fifteen professions, including the medical profession, mention only the Treaty and/or the arguably non-Tiriti compliant Treaty principles. This Crown construction effectively fails to address the actual undertakings embodied in te Tiriti. Only one profession, occupational therapy, orients to both te Tiriti and the Treaty of Waitangi and does not default to Treaty principles.
Phase two: competency close examination
In a CTA, each of the five te Tiriti domains has an indicator to help assess compliance. These domains are explored more fully elsewhere.16 They are adapted here to relate specifically to competencies.
Preamble
Te Tiriti is central and Māori are equal or lead parties
Several of the competency documents acknowledged Māori as tangata whenua—people of the land. The Dieticians Board17 noted: “Māori as Tangata Whenua hold a unique place in our country.” Some competencies referenced the importance of relationships with Māori, and others extended their reference to include relationships with iwi (tribes), hapū and whānau (extended family). The Occupational Therapy Board explicitly refer to the identification of OT’s role in “in building and sustaining relationships with whānau, hapū, iwi, Māori organisations and tangata whenua as a whole.”18
Article 1
Mechanisms to ensure equitable participation and/or leadership
It was often unclear from the core competency documents how Māori were involved in competency development and/or in leadership of professional bodies.
Article 2
Evidence of Māori values influencing the competencies
Some of the competency documents specifically referenced the importance of tikanga (Māori protocol) and Māori health models. The competency documents rarely included key Māori concepts such as manaakitanga (to care for), tika (doing things the right way), pono (to act with integrity) or aroha (love). Some recognised the importance of whānau groupings to Māori.
Article 3
Evidence of Māori exercising their citizenship as Māori
The Occupational Therapy Board18 recognised the “history, cultures, and social structures influencing health.” Several competency documents noted a requirement to be committed to the pursuit of positive Māori health outcomes.
Article 4
Acknowledgement of the importance of wairua, rongoā and wellbeing
Wairua and spiritual wellbeing were mentioned in the context of the Māori health model Te Whare Tapa Whā.1 Rongoā was rarely mentioned.
Phase three: competency determination
The CTA determination (Table 2) was based on the information presented in the competency documents. We applied the CTA assessment criteria in the following ways:
- Poor: The competency documented substantially failed to transparently address the indicator.
- Fair: The core competencies have vague engagement with the indicator (eg, acknowledgement of culture).
- Good: The competencies appear to deliberately and consciously address the criteria (eg, acknowledgement of tikanga).
- Excellent: The core competencies clearly achieve the indicator (eg, acknowledgement of power-sharing).
Table 2: Regulated health professions mapped against articles of the Māori text (te Tiriti).

Poor: 0. Fair: 1. Good: 2. Excellent: 3.
The chiropractic,19 medical radiation technology20 and physiotherapy21 core competencies cover both Australia and Aotearoa and contain no evidence of Māori input into their development. Similarly, the osteopathic competencies22 were developed by Australian academics. Te Ao Mārama (the Māori Dental Association) is mentioned in the dental competencies23 but without clarification of their input. The core competencies of the dietitians17 were developed by an expert working group with Māori representation. Likewise, a designated committee of the Psychologists Board24 developed their competencies, although Māori input into that process is unclear. The Medical Sciences Council25–26 and the Medical Council27 regularly review competencies they administer, which includes an undefined public consultation process. The Midwifery Council,28 Nursing Council,29–31 Optometrist and Dispensing Opticians Board,32 Social Workers Registration Board,33 Podiatry Board,34 Psychotherapists Board,35 Pharmacy Council36 and Occupational Therapy Board18 offer no detail of how they developed their competencies.
Those practitioner competencies that scored ‘excellent’ when assessed against the preamble18,21,24,29–31,36 did so due to in part to the requirement for practitioners to demonstrate relevant application of te Tiriti/Treaty in their practice. Each also acknowledged Māori as partners. The Pharmacy Council36 in particular articulated the importance of te Tiriti for practitioners, by emphasising that:
“Learning about the impact of pre- and post-Te Tiriti o Waitangi events on the health of New Zealanders and developing working relationships with key Maori stakeholders e.g. Iwi / Hapū -/ Whānau / Māori organisations, where appropriate, will provide background to help improve Māri health outcomes. This extends to understanding the contemporary application of Te Tiriti o Waitangi.”
The Pharmacy Council also provided a clear acknowledgement of the importance of Māori models of health and practices, such as tikanga and kawa, in contributing to improved relationships and health outcomes, which contributed to their excellent score for the Article 4 indicator.
Discussion
Phase four: strengthening practice
The WAI 2575 report12 gave the health sector a collective ‘D grade’ for our failure to perform in relation to Māori health. To deliver health services effectively, health practitioners need to have the necessary clinical, cultural and political skills to engage effectively with whānau. Following on from the work of Heke, Wilson and Came,14 which highlighted the need to strengthen and synthesise cultural competencies, this study suggests that existing professional competency documents are not yet fit for purpose as frameworks for upholding te Tiriti.
A te Tiriti-compliant health sector requires legislation, policy, competency documents, standards, codes of ethics and relevant supplementary documents to explicitly uphold te Tiriti. Individuals, teams, disciplines and organisations would all be held accountable for their inaction and action. Competencies could have explicit statements about knowledge and understanding of the cultural, historical, political and social context of Aotearoa, including the importance of te Tiriti o Waitangi and He Whakaputanga o te Rangatiratanga o Nū Tīreni (the New Zealand Declaration of Independence). The Pharmacy Council integrated into their competencies the importance of understanding and being able to describe the relevance of te Tiriti while also understanding Māori perspectives of health and the ability to incorporate strategies to address disparities.36 Similarly, the Physiotherapy Board requires the ability to “demonstrate contemporary application of te Tiriti principles and the incorporation into practice of the four cornerstones of health.”21 Berghan, Came, Doole, Coupe, Fay, McCreanor and Simpson5 have argued that upholding te Tiriti requires three key elements: (i) whakawhanaungatanga (the active making of relationships with Māori), (ii) tauiwi (settler people) consciously becoming an ally with Māori in the pursuit of racial justice and (iii) actively engaging in decolonisation or power-sharing. The Occupational Therapy Board and Pharmacy Council both begin to articulate these elements in statements that detail meeting and developing relationships with the Māori health, welfare and education workforce18 and practising whanaungatanga to build relationships and trust with key partners.36 These complex processes may not be captured seamlessly in a traditional competency document. However, this difficulty doesn’t mean that competency development shouldn’t attempt a deeper engagement with the five domains of the Māori text.
Table 3 offers some specific ideas for te Tiriti competencies that could be refined and integrated into core competency documents. These competencies could be tailored into professional development plans for individual practitioners or teams, recognising pre-existing expertise. The competencies could be staircased into preliminary, secondary and advanced competencies, similarly to the Pharmacy Council’s competency structure, which includes a continuum of professional development.36
Table 3: Possible te Tiriti o Waitangi competencies for tauiwi.5
As a methodological note, we acknowledge that the decision to use only core competency documents in our analysis may not reflect well for those professions who handle te Tiriti and/or the Treaty and/or Treaty principles differently. We note that all reviewed professions, except osteopaths and social workers, have separate cultural competencies where references to te Tiriti and/or the Treaty might have been more prolific. However, we argue that the rightful position of te Tiriti in health is at the core, not on the periphery.
Phase five: Māori final word
For Māori, health is a complex concept that incorporates elements of health, vitality and wellbeing as well as illness, disease and malaise. These all occur within the contexts of connection to each other, ancestors and the environment, with the whole package being acknowledged as taonga. Māori health aspirations are effectively captured within the text of te Tiriti o Waitangi, including Māori leadership and agency, practices that centre the Māori worldview and the valuing of Māori approaches to health and wellbeing.
Health professionals occupy intimate spaces in Māori lives, as they do with all citizens, whether they are promoting good health, protecting communities and individuals from poor health or caring for the sick. It is vital that the work of health professionals is aligned with the full health aspirations of Māori as outlined in te Tiriti.
This analysis of competency documents of regulated health professionals has highlighted the various ways different professional groups have incorporated te Tiriti into their practice. The majority of the professions are not meeting their obligations as a Crown Tiriti partner. It is not a stretch to posit that this is a contributing factor to the poor health outcomes and racism that Māori experience when seeking healthcare. The current competency documents clearly show that Māori health aspirations and te Tiriti obligations are not being considered, much less achieved, in Aotearoa.
Authors
Heather Came: Head of Department – Public Health, Faculty of Health and Environmental Sciences, Auckland University of Technology. Jacquie Kidd: Associate Professor Jacquie Kidd, Faculty of Health and Environmental Sciences, Auckland University of Technology. Deborah Heke: PhD Candidate, Taupua Waiora Centre for Maori Health Research, Faculty of Health and Environmental Sciences. Tim McCreanor: Te Rōpū Whāriki, Massey University, Auckland.Acknowledgements
Thanks to the hard-working practitioners who pulled together their professional competency documents. We wish you well in the ongoing efforts to refine and improve these documents so te Tiriti o Waitangi can be upheld and anti-racism praxis be normalised.Correspondence
Heather Came: Head of Department – Public Health, Faculty of Health and Environmental Sciences, Auckland University of Technology, Private Bag 92006, Auckland 1142, +64 9 921 9999 ext 7799Correspondence email
heather.came@aut.ac.nzCompeting interests
Nil.1. Durie M. Whaiora: Māori health development. 2nd ed. Auckland, New Zealand: Oxford University Press; 1998.
2. Anderson I, Robson B, Connolly M, Al-Yaman F, Bjertness E, King A, et al. Indigenous and tribal peoples' health (The Lancet–Lowitja Institute Global Collaboration): a population study. The Lancet. 2016;338(10040):131-57.
3. Moewaka Barnes H, McCreanor T. Colonisation, hauora and whenua in Aotearoa. Journal of the Royal Society of New Zealand. 2019;49(sup1):19-33.
4. United Nations. Declaration on the Rights of Indigenous Peoples. New York, NY: Author; 2007.
5. Berghan G, Came H, Doole C, Coupe N, Fay J, McCreanor T, et al. Te Tiriti-based practice in health promotion. Auckland, New Zealand: STIR: Stop Institutional Racism; 2017.
6. Healy, Huygens I, Murphy T. Ngāpuhi speaks. Whangarei, New Zealand: Network Waitangi Whangarei, Te Kawariki; 2012.
7. Hayward J. The principles of the Treaty of Waitangi. In: Ward A, editor. Rangahau whanui national overview report. Wellington, New Zealand: Waitangi Tribunal; 1997. p. 475-94.
8. Royal Commission on Social Policy. The April report 2. Wellington, New Zealand: Author; 1988.
9. Came H, Cornes R, McCreanor T. Treaty of Waitangi in New Zealand public health policy 2006-2016 New Zealand Medical Journal. 2018;131(1469):32-27.
10. Cabinet Office. Te Tiriti o Waitangi/ Treaty of Waitangi guidance Wellington, New Zealand: Author; 2019 [Available from: https://dpmc.govt.nz/sites/default/files/2019-10/CO%2019%20%285%29%20Treaty%20of%20Waitangi%20Guidance%20for%20Agencies.pdf.
11. Waitangi Tribunal. He Whakaputanga me te Tiriti - The Declaration and the Treaty [WAI 1040]. Wellington, New Zealand: Author; 2014.
12. Waitangi Tribunal. Hauora report on stage one of the health services and outcomes inquiry. Wellington, New Zealand: Author; 2019.
13. Health and Disability System Review. Health and Disability System Review – Final Report – Pūrongo Whakamutunga. Wellington, New Zealand: Author; 2020.
14. Heke D, Wilson D, Came H. Shades of competence? A critical analysis of the cultural competencies of the regulated-health workforce in Aotearoa New Zealand. International Journal for Quality in Health Care. 2018:mzy227-mzy.
15. Came H, O'Sullivan D, McCreanor T. Introducing Critical Tiriti Analysis through a retrospective review of the New Zealand Primary Health Care Strategy Ethnicities. 2020.
16. Came H, Kidd J, Goza T. A critical Tiriti analysis of the New Zealand Cancer Control Strategy. Journal of Cancer Policy. 2020:100210.
17. Dietitians Board. Professional standards and competencies for dietitians. Wellington, New Zealand: Author; 2017.
18. Occupational Therapy Board of New Zealand. Competencies for registration and continuing practice. Wellington, New Zealand: Author; 2015.
19. New Zealand Chiropractic Board. Competency-based professional standards for chiropractors. Wellington, New Zealand: Author; 2010.
20. New Zealand Medical Radiation Technologists Board. Competence standard for medical imaging and radiation therapy practice in New Zealand. Wellington, New Zealand: Author; 2017.
21. Physiotherapy Board of Australia, Physiotherapy Board of New Zealand. Physiotherapy practice thresolds in Australia and Aotearoa New Zealand. Australia: Authors; 2015.
22. Stone C, Hager P, Boud D. Capabilities for osteopathic practice. Sydney, Australia: Osteopathic Council of New Zealand; 2009.
23. Dental Council. Working as an oral health practitioner in New Zealand: Handbook for the New Zealand conditions of practice. Wellington, New Zealand: Author; 2011.
24. New Zealand Psychologists Board. Core competencies for the practice of psychology in New Zealand. Wellington, New Zealand: Author; 2011.
25. Medical Sciences Council of New Zealand. Competencies standards for anaesthetic technicians in Aotearoa New Zealand. Wellington, New Zealand: Author; 2018.
26. Medical Sciences Council of New Zealand. Competencies standards for medical laboratory science practitioners in Aotearoa New Zealand. Wellington, New Zealand: Author; 2018.
27. Medical Council of New Zealand. Good medical practice. Wellington, New Zealand: Author; 2016.
28. Midwifery Council of New Zealand. Statement of clinical and cultural competencies for midwives. Wellington, New Zealand: Author; 2007.
29. Nursing Council New Zealand. Competencies for registered nurses. Wellington, New Zealand: Author; 2007.
30. Nursing Council New Zealand. Competencies for enrolled nurses. Wellington, New Zealand: Author; 2012.
31. Nursing Council New Zealand. Competencies for the nurse practitioner scope of practice. Wellington, New Zealand: Author; 2017.
32. Optometrists and Dispensing Opticians Board. Standards of clinical competence for dispensing opticians. Wellington, New Zealand: Author; 2018.
33. Social Workers Registration Board. The SWRB ten core competence standards. Wellington, New Zealand: Author; 2003.
34. Podiatrists Board of New Zealand. Principles and standards for the practice of podiatry in New Zealand. Wellington, New Zealand: Author; 2019.
35. The Psychotherapists Board of Aotearoa New Zealand. The Pscyhotherapists Board of Aotearoa New Zealand Psychotherapist core clinical competencies. Wellington, New Zealand: Author; 2010.
36. Pharmacy Council of New Zealand. Competence standards for the pharmacy profession. Wellington, New Zealand: Author; 2015.
37. Durie M. Te pae mahutonga: A model for Māori health promotion. Health Promotion Forum Newsletter. 1999;49:2-5.
38. Hudson M, Milne M, Reynolds P, Russell K, Smith B. Te ara tika guidelines for Māori research ethics: A framework for researchers and ethics committee members. Wellington, New Zealand: Health Research Council; 2010. 29 p.
